Intracorneal knot or flange depot fixation: new transscleral technique for intraocular lens fixation.

Abstract
A new surgical technique of transscleral-intracorneal suture fixation of intraocular lenses with suture ends located within the transparent corneal or corneal–limbal paracentesis is reported. This new technique significantly reduces scleral and conjunctival trauma, is minimally invasive, is simple to perform, is not associated with complicated intraocular surgical maneuvers, and precludes suture knot, flange, and suture-end erosion. The internal part of the corneal stroma or corneal–limbal area serves as a secure depot for suture-end fixation with durable resistance. The technique enables visualization of the exact position of suture ends over time.
Multiple surgical techniques for posterior chamber intraocular lens (PC IOLs) implantation in the absence of adequate capsular support are currently used. Sutureless intrascleral fixation, iris fixation suture, and transscleral fixation with knot or knotless techniques and their numerous modifications have been described.1–4 Visual rehabilitation after both sutured and sutureless techniques appear equally effective.5 Therefore, technique choice is determined by comorbidities and individual surgeon preference rather than by proof of superiority. Transscleral suture fixation, especially for late in-the-bag PC IOL dislocation, is an easy and fast approach when IOL exchange is considered higher risk. Potential suture erosion drives both the choice of suture material and the need for scleral flap formation, large conjunctival dissections for the z-suture technique, or additional traumatic manipulations.4 Our proposed technique of transscleral-intracorneal (TS-IC) knot or flange depot fixation is efficient and simple and precludes knot or flange erosion leading to serious late complications including endophthalmitis.
SURGICAL TECHNIQUE
This PC IOL fixation technique uses 9-0 or 10-0 polypropylene suture. GoreTex, used by some (off-label) for scleral fixation, is not applicable because of its larger diameter and slippery nature. Gentian violet (pen or stained spatula) is used to make limbal horizontal marks 180 degrees apart along the target meridian centered on the optical axis. Two transconjunctival sclerotomy sites are marked 2.5 mm from the limbus peripheral to the horizontal markings. A corneal stab incision (paracentesis) is performed using a 20-gauge MVR knife (MV2 20, Mani, Inc., or Beaver-Visitec International, Inc.) corresponding to the location of the sclerotomy marking (Figure 1, A) and is preserved exclusively for the final suture location and not for manipulations with microsurgical instruments. Additional corneal incisions may be made to approach and keep the chamber formed by an anterior chamber maintainer or ophthalmic viscosurgical device or any other preferred means.
Next, a 25-gauge guide needle is passed ab externo through the distal sclerotomy site, under the subluxated bag-lens complex or implant trapping a haptic or capsular tension ring and is used to dock the tip of the single-armed 9-0 or 10-0 polypropylene 15 mm side-cut needle with loop suture (2452-L or 2451-L, Mani, Inc.) (Figure 1, B) introduced through the corneal paracentesis. The tip is externalized through conjunctiva (Figure 1, C). A nonlooped suture may be used as well. To assure the conjunctival and scleral entry points are noncoincident, the conjunctiva is then grasped with atraumatic conjunctival forceps or a spatula and stretched for 0.3 mm while holding the partially externalized needle tightly from inside the anterior chamber, and the conjunctiva is moved in the opposite direction. Large conjunctival dissection may be avoided as the initial penetration of the 25-gauge needle forms a round conjunctival incision that, when stretched in the right direction prior to initial entry, serves as a convenient location for needle reinsertion into sclera later.
The needle is then completely externalized and grasped by the tip approximately 0.3 mm peripheral to the sclerotomy site (Figure 1, D) and passed transsclerally and transcorneally (through the half depth of the previous corneal incision) (Figure 1, E). Afterward, it is then externalized through nearby cornea just superior to the paracentesis (Figure 1, F). Then, the needle is cut off, and the sutures are retrieved through the corneal incision with a Sinskey hook in a similar manner to the Hoffman pocket technique.6 Alternatively, a faster method to externalize the sutures is to use a reverse needle maneuver, passing hub-first through the corneal paracentesis.
Once the IOL is centered in the pupillary plane by appropriate suture tightening, there are several approaches for tying the knot. The 9-0 polypropylene suture knot security is achieved with a 2-1-1 throw knot, allowing titration of tension for IOL centration (Figure 1, G and H). The completed knot is fully buried in the corneal paracentesis within the stroma (Figure 1, I). If a 10-0 polypropylene single-armed suture is used, the recommended suture configuration is 2-1-1-1. This added final throw increases the overall diameter of the knot ideally. The knot is tied to allow the paracentesis roof and floor to appose in their normal anatomic position to seal the incision with the knot secured within, well away from the initial entry site of the 2452-L needle (Mani, Inc.). The surgical technique is demonstrated in Figure 2 and Video 1 (available at https://links.lww.com/JRS/A581).
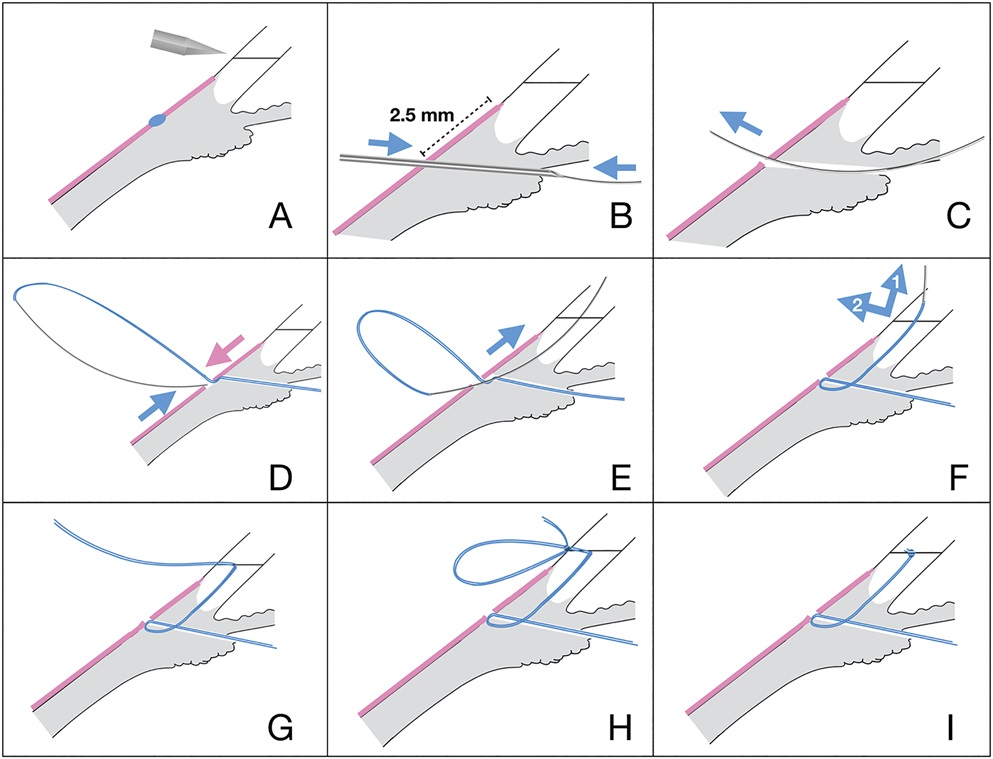
Figure 1.: Schematic representation of the main steps of the transscleral-intracorneal knot depot fixation technique. The blue arrows indicate the needle direction and the pink arrows the direction of conjunctival displacement. A: A keratome corneal stab incision is performed in the meridian anterior to the sclerotomy penetration site. B: The 25-gauge guide needle is passed ab externo through the sclerotomy site and under the subluxated bag-lens complex and is used to dock the 9-0 polypropylene curved suture needle. C: The needle tip is externalized. D: The needle is inserted ∼0.3 mm peripherally and to the side of the sclerotomy site by gently moving the conjunctival hole with the microforceps, so that the small part of the suture on the scleral surface is covered by conjunctiva. E: The curved needle is passed upward through the sclera and then transcorneally through the middle of the corneal paracentesis exiting the cornea. F and G: The needle is pushed transcorneally by the needle holder grasping the tip external to the corneal surface and guided backward until the swaged end is located at the level of the corneal paracentesis, allowing it to be externalized through the corneal paracentesis by reverse movement (the numbers in the arrows indicate a sequence of manipulations). H: The knot is securely tied by 2-1-1 technique and buried inside the corneal incision. I: The residual suture is cut off, and the knot is placed intracorneally within the paracentesis.
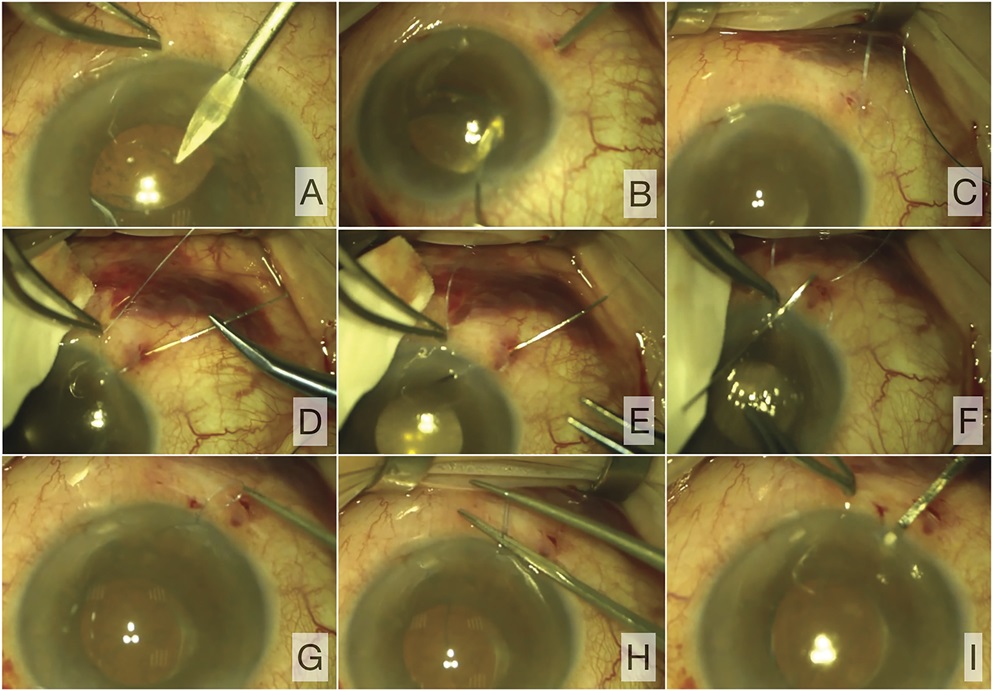
Figure 2.: Intraoperative view of the main steps of the transscleral-intracorneal knot depot fixation technique. A: A stab corneal incision is performed using a keratome corresponding to the location of the future sclerotomy marking (the transscleral suture passage). B: The 25-gauge guide needle is passed ab externo through the sclerotomy site and is used to dock the tip of the 9-0 polypropylene curved suture needle. C: The needle is externalized. D, E: The needle located by the tip ∼0.3 mm peripheral to the sclerotomy site is passed transsclerally-transcorneally through the half depth of the corneal paracentesis to exit on the corneal surface. F: The swaged end of the needle is than externalized by reverse movement of the needle through the corneal paracentesis. G, H: The knot is securely tied by a 2-1-1 technique once the IOL-bag complex is in the ideal centered position. I: The residual ends having been cut off, the knot is tucked intracorneally within the paracentesis with the microsurgical spatula.
Flanged technique is an alternative to knot corneal suture fixation (Figure 3; Video 2 available at https://links.lww.com/JRS/A582). The double 9-0 polypropylene suture is externalized and fixed with the needle holder forceps with a little tension just inside the corneal paracentesis so that the distal part of the suture 2.5 to 4.0 mm in length is external for cauterization and the rest is cut off. Caution must be taken to unite the suture ends, so that the 2 distal threads are equal in size and stuck together with balanced salt solution to be melted into 1 flange. Cautery is used to melt the suture ends just up to the securing instrument holding them to avoid any effect on the corneal tissue. The suture ends are thereby fused into 1 flange by cauterization, and the flange is then buried into the corneal stroma in a similar fashion to the knot by pushing it into the paracentesis.
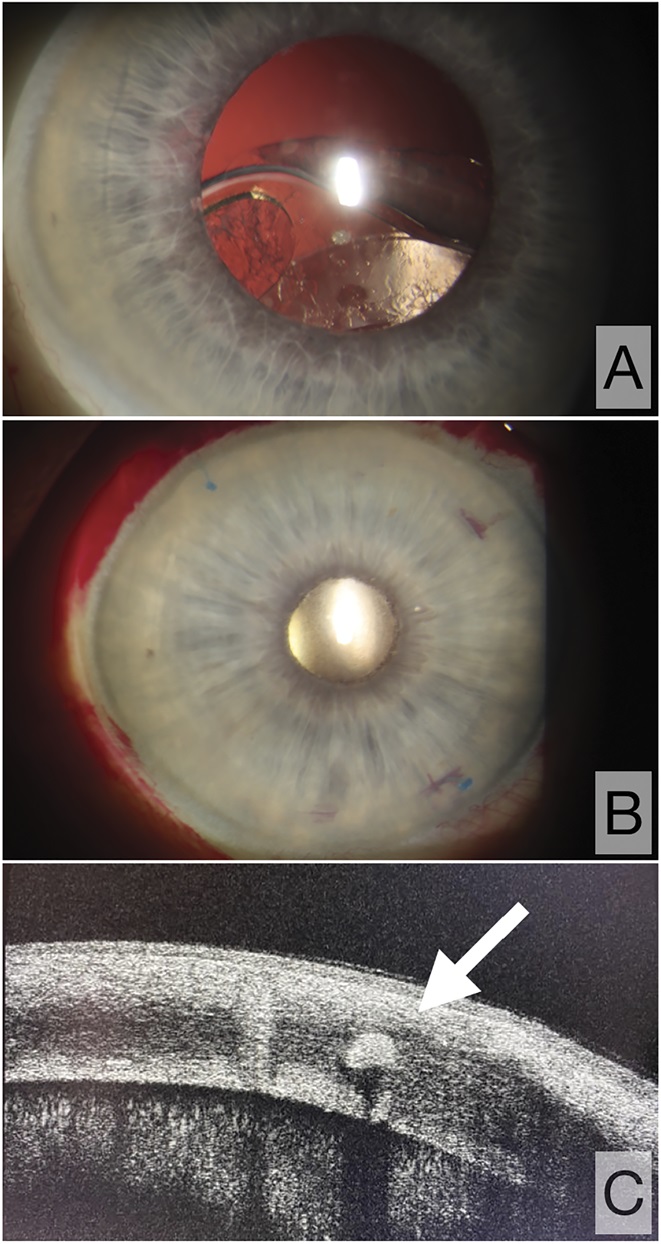
Figure 3.: Slitlamp biomicroscopic view. A: Preoperative view of the anterior segment: in-the-bag IOL dislocation. B: Postoperative view of the anterior segment after IOL fixation surgery with transscleral-intracorneal flange depot fixation technique: well-centered IOL, suture flange (2 ends fused into 1 flange) buried intracorneally. C: OCT scan at the 11-clock hour showing the flange located within the corneal stroma.
RESULTS
This retrospective study included 36 eyes of 35 patients (19 men, 16 women; mean age 72.1 years ± 11.7 [SD]). The surgery was performed by 2 surgeons (A.A.K., N.S.A.). The TS-IC suture fixation of acrylic hydrophobic and hydrophilic 1-piece IOLs was combined with additional procedures due to a diversity of comorbidities (Table 1). The postoperative follow-up time was 16.9 months ± 11.1 (median 11 months, minimum 1 month, and maximum 12 years). Intraoperative and postoperative complications are summarized in the Table 2.
| No additional procedures, n | 16 |
| Phacoemulsification, n | 1 |
| NPDS with XCB-CGI, n | 2 |
| Trabeculectomy, n | 3 |
| Anterior vitrectomy, n | 2 |
| Anterior vitrectomy with intravitreal anti-VEGF injection, n | 1 |
| Intravitreal anti-VEGF injection, n | 1 |
| IOL exchange, n | 1 |
| IOL exchange, 25-gauge vitrectomy with CTR removal from vitreal cavity, n | 1 |
| Secondary IOL implantation in aphakia, n | 3 |
| 25-gauge vitrectomy, n | 1 |
| 25-gauge vitrectomy with internal limiting membrane peeling, n | 3 |
| 25-gauge vitrectomy with endolaser retina photocoagulation, 5700 cSt silicone oil injection, n | 1 |
| Transient IOP elevation, n (%) | 6 (17) |
| Transient corneal edema, n (%) | 3 (8) |
| Corneal epithelial erosion, n (%) | 3 (8) |
| Persistent rise in IOP, n (%) | 1 (3) |
| Partial hemophthalmus, n (%) | 1 (3) |
| Epiretinal membrane, n (%) | 1 (3) |
| IOL tilt | — |
| Secondary IOL dislocation requiring intervention | — |
| Bullous keratopathy | — |
In the early postoperative period, the baseline intraocular pressure (IOP) increased to 25.8 mm Hg ± 1.5 (SD) in 6 patients (16%) (the baseline IOP increased by 5.8 mm Hg ± 2.6). Five of the 6 patients had IOP stabilized to presurgical pressure by 2 weeks postoperatively. Of these, 3 patients had open-angle glaucoma and were on 2 topical hypotensive medications preoperatively. One patient required surgical intervention (nonpenetrating deep sclerotomy with a xenogenically derived cancellous bone glaucoma implant) within 1 month of IOL fixation surgery due to topical treatment-resistant IOP elevation and open-angle glaucoma.7 Intraoperative complications were seen in only 1 case where vitreous hemorrhage occurred and completely resolved within 2 weeks without additional surgical intervention. One case of epiretinal membrane formation occurred 3 months after IOL fixation surgery. This patient's subsequent 25-gauge vitrectomy with internal limiting membrane peel provided a good functional outcome. Corrected distance visual acuity improved significantly in all cases after IOL fixation surgery (preoperatively and 1 month postoperatively corrected distance visual acuity 0.36 ± 0.20 and 0.19 ± 0.18 (logMAR), respectively, P < .01). TS-IC fixation technique resulted in long-term anatomic success in all cases. None required repeat IOL fixation in the follow-up time. None demonstrated knot or flange erosion. The most frequent complication overall was a transient IOP rise presumed due to retained ophthalmic viscosurgical device.
DISCUSSION
The TS-IC knot or flange depot fixation technique offers multiple advantages over previously described techniques. Primarily, there is no need for extensive conjunctival dissection or scleral coagulation, which can be limited to the needle passage site (less than 1 mm in diameter) only. The technique is useful for fixating various intraocular implants such as IOLs, artificial iris prostheses, and conventional or modified capsular tension rings by any preferred technique including lasso, cow-hitch, or modified cow-hitch.8–10 It is applicable to any number of fixation points as the individual case dictates (2-, 3-, 4-point fixation). Special equipment is limited to the appropriate curved 15 mm side-cut needle with one-fourth circle 90-degree curvature, which simplifies suture passage in the right direction through the half-depth corneal paracentesis and its subsequent easy reversal to externalize it directly through this preprepared corneal incision. The larger size (9-0) polypropylene suture is preferable to delay possible suture surface biodegradation shown to occur in highly vascularized tissue.11
Intracorneal knot construction is an integral aspect of the technique because of the unyielding nature of the cornea. Since the knot serves as an anchor, the diameter of the suture is required to be more than the suture channel created by the needle to remain secure. If too bulky, it risks paracentesis gape in the early-postoperative period. With the technique as described, we have seen no leaks from the paracentesis in early or late follow-up. Although our experience is with a full-thickness manual corneal paracentesis incision for secure fixation of the knot, the femtosecond laser, capable of creating a precise nonpenetrating intracorneal incision sufficient to contain the TS-IC suture fixation, may prove efficacious in the future.
The main advantage of this new technique where the corneal incision serves as the knot or flange depot is the absence of knots and flanges in the area where the conjunctiva corresponds to the suture passage in sclera, thereby completely excluding suture erosion, known to be the main late complication of transscleral-sutured intraocular implants in other techniques. Even scleral flaps and grooves still allow suture erosion in 73% of patients at a mean postoperative time of 9.4 months.12 In addition, eyes with scleral thinning associated with previous surgery or trauma may preclude safe creation of scleral flaps. Although scleral patching and corneal autografts have been shown to prevent knot erosion, this method is unreasonably time-consuming and invasive and has not gained popularity.13 Zigzag-shaped (z-suture) intrascleral suture technique was introduced to avoid knot erosion and replaced the obsoleted scleral flaps.4 Although this knotless technique has been shown in a retrospective study to avoid conjunctival erosion in the long-term, it requires extensive conjunctival dissection, especially in 4-point z-suture fixation.14,15 Conjunctival sparing, particularly in patients with a filtering bleb near the fixation meridian or who may require future glaucoma surgery, is desirable for optimal outcomes.16 Similarly, the Hoffman pocket technique may reduce the efficacy of scleral glaucoma procedures as it involves 30-degree (1-clock hour) intrascleral incision, although the conjunctiva is less effected by fibrotic reaction when the limbal-based approach is used.6 Our other proposed flange modification for stable fixation of the suture ends using the cornea for its depot (Figure 3, C) has been previously described only transsclerally.17
The TS-IC technique provides a stable, durable position for the suture knot or the flanged end of the suture that is easily visualized during long-term postoperative observation (the maximum follow-up is 12 years in our experience). Neither the suture knot or the flange protrudes through the cornea in any direction. Avascular corneal tissue induces minimal biodegradation and avoids suture breakage. This new suturing technique offers a viable alternative for safe transscleral fixation of various types of intraocular implants.
WHAT WAS KNOWN
- Implant scleral fixation is performed with knot, flange, or suture end fully or partially subconjuctival or intrascleral.
- Transconjuctival suture end erosion may occur when using transscleral suture fixation resulting in serious late complications.
WHAT THIS PAPER ADDS
- Transscleral-intracorneal (TS-IC) is useful for fixating various intraocular implants by any preferred technique including lasso, cow-hitch, or modified cow-hitch.
- TS-IC obviates the need for extensive conjunctival dissection or scleral coagulation.
- Intracorneal knot or flange depot fixation excludes the risk for suture end erosion.
REFERENCES
1. Gabor SGB, Pavlidis MM. Sutureless intrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg 2007;33:1851–1854
2. Chang DF. Siepser slipknot for McCannel iris-suture fixation of subluxated intraocular lenses. J Cataract Refract Surg 2004;30:1170–1176
3. Smiddy WE, Sawusch MR, O'Brien TP, Scott DR, Huang SS. Implantation of scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg 1990;16:691–696
4. Szurman P, Petermeier K, Aisenbrey S, Spitzer MS, Jaissle GB. Z-suture: a new knotless technique for transscleral suture fixation of intraocular implants. Br J Ophthalmol 2010;94:167–169
5. Sindal MD, Nakhwa CP, Sengupta S. Comparison of sutured versus sutureless scleral-fixated intraocular lenses. J Cataract Refract Surg 2016;42:27–34
6. Hoffman RS, Fine IH, Packer M. Scleral fixation without conjunctival dissection. J Cataract Refract Surg 2006;32:1907–1912
7. Anisimova NS, Arbisser LB, Anisimov SI, Arutyunyan LL, Shilova NF, Bashaeva G, Kirtaev RV, Anisimova SY. Five-year results of non-penetrating deep sclerectomy with demineralized cancellous bone xenogenically derived collagen glaucoma implant. Int Ophthalmol 2021;41:2041–2052
8. Stevens JD, Hamilton AM. Displaced intraocular lens repositioning using a reversed 10-0 straight polypropylene needle lasso technique. Br J Ophthalmol 1993;77:390
9. Nakashizuka H, Shimada H, Iwasaki Y, Matsumoto Y, Sato Y. Pars plana suture fixation for intraocular lenses dislocated into the vitreous cavity using a closed-eye cow-hitch technique. J Cataract Refract Surg 2004;30:302–306
10. Chen SX, Lee LR, Sii F, Rowley A. Modified cow-hitch suture fixation of transscleral sutured posterior chamber intraocular lenses: long-term safety and efficacy. J Cataract Refract Surg 2008;34:452–458
11. Price MO, Price FW, Werner L, Berlie C, Mamalis N. Late dislocation of scleral-sutured posterior chamber intraocular lenses. J Cataract Refract Surg 2005;31:1320–1326
12. Solomon K, Gussler JR, Gussler C, Van Meter WS. Incidence and management of complications of transsclerally sutured posterior chamber lenses. J Cataract Refract Surg 1993;19:488–493
13. Bucci FAJ, Holland EJ, Lindstrom RL. Corneal autografts for external knots in transsclerally sutured posterior chamber lenses. Am J Ophthalmol 1991;112:353–354
14. Dimopoulos S, Dimopoulos V, Blumenstock G, Trevino-Rodriguez H, Bartz-Schmidt KU, Spitzer MS, Voykov B. Long-term outcome of scleral-fixated posterior chamber intraocular lens implantation with the knotless Z-suture technique. J Cataract Refract Surg 2018;446:182–185
15. Spitzer MS, Yoeruek E, Leitritz MA, Szurman P, Bartz-Schmidt KU. A new technique for treating posttraumatic aniridia with aphakia: first results of haptic fixation of a foldable intraocular lens on a foldable and custom-tailored iris prosthesis. Arch Ophthalmol 2012;130:771–775
16. Murchison JF Jr, Shields MB. Limbal-based vs fornix-based conjunctival flaps in combined extracapsular cataract surgery and glaucoma filtering procedure. Am J Ophthalmol 1990;109:709–715
17. Hu XT, Zhang ZD, Zhou R, Pan QT. Cauterization technique for suture erosion in transscleral fixation of intraocular lenses. Int J Ophthalmol 2013;6:892–894
Ссылка на источник: https://journals.lww.com/jcrs/Fulltext/2022/06000/Intracorneal_knot_or_flange_depot_fixation__new.19.aspx?context=FeaturedArticles&collectionId=1
Назад в «Готовятся к публикации»